









Development of symptoms in meningococcal disease - new research on pre-admission symptoms
The study which provided the clinical cases for this learning tool also collected data on the pre-admission symptoms of 448 children aged less than 17 years. Parents were asked to report the time the illness first started, the initial symptom and all subsequent symptoms until hospital admission.
There has been very little information in the recent literature on this subject to guide doctors; published information about the development of symptoms generally relies on data collected from hospital patients. The results of this study provide the first description of the time course of the clinical features of meningococcal disease in children and adolescents prior to hospital admission
Recognition of meningococcal disease can be difficult especially for doctors unfamiliar with the infection. Doctors may rely on the text book image of advanced meningococcal disease or look for symptoms more often reported in adults like neck stiffness and photophobia. It also does not help that doctors, parents and the media call this disease meningitis and so the importance of septicaemia is ignored or forgotten.
The full paper describing the pre-admission symptoms of the patients can be read in full in the Lancet7. A summary of the important finding is shown below.
Clinical features of disease
Table 1 shows all the symptoms reported by parents and the median time it took for those symptoms to appear from the start of this illness. The children are grouped into 4 age bands as children within each age band have similar case fatality rates. The red lines in each column show the median time it took parents to take their child to a GP. From the table it can be seen that it takes longer for older children to be taken to the doctor. This could be because their symptoms take longer to manifest or that their parents are less worried about them and respond less quickly.
Earliest symptoms
The earliest features were common to many self-limiting viral illnesses. Fever was the first symptom to be noticed in children aged under 5 years, headache in the older children and adolescents. Virtually all children (95%) developed fever at some point and most young children were miserable and irritable. Anorexia, nausea and vomiting were relatively early features at all ages, with many children also exhibiting upper respiratory symptoms (sore throat and coryza). This non-specific phase lasted for about 4 hours in younger children but as long as 8 hours in adolescents.
Sepsis symptoms
The next symptoms to develop in all age groups were signs of sepsis and circulatory shut-down – limb pain, abnormal colour, cold extremities and, in older children, thirst. Parents of younger children also reported drowsiness and breathing difficulty (usually described as rapid or laboured breathing) at this stage and occasionally diarrhoea.
Three symptoms were fairly frequent : cold extremities (35-47%), limb pain (31 -63% excluding infants) and abnormal colour (17-21%), usually described as pallor or mottling. Thirst, diarrhoea and breathing difficulty presumably also reflect sepsis but were less common.
Rash
The first classic symptom to emerge was rash, although at onset this was sometimes non-specific and only evolved to a petechial and then grossly haemorrhagic rash over a period of hours. Although it was the most common classic feature of disease it was certainly not always present. (see table2). In infants a haemorrhagic rash was present in less than half of cases by hospital admission. The rash was also not an early symptom occurring a median of 8hours after the start of the illness in babies, 9 hours in 1-4 year olds, 14 hours in 5-14 year olds and 19 hours in the 15 and 16 year olds.
Symptoms of meningitis
Meningism was more common in older children, about half the children aged over 5 years had symptoms of meningism and half of these had photophobia. These are not reliable signs in children below 5 years of age.
The median time of onset of specific symptoms suggestive of meningitis (neck stiffness, photophobia, bulging fontanelle) was later, around 12-15 hours from illness onset. The very late stage signs (such as unconsciousness, delirium, or seizures) occurred at a median of 15 hours in infants, about 24 hours in older children.
Fig 1. Time course of development of symptoms.
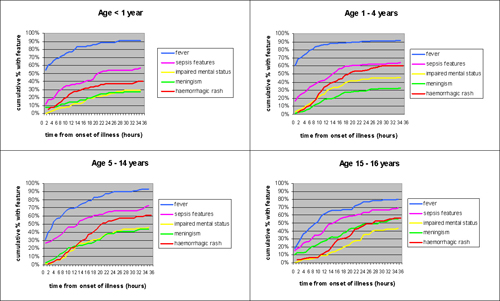
Click the image for a larger version
Figure 1 displays graphically by age group the proportion of children developing specific groups of symptoms over the 36 hours from onset of illness. It shows that few children develop new symptoms after 24 hours from onset .The order of progression at all ages is fever, sepsis symptoms and then the classic symptoms of haemorrhagic rash, impaired mental state and meningism. The slower progression of illness in the oldest children is clear; they are also the only age group in which meningism is an earlier and more frequent feature than haemorrhagic rash and impaired consciousness.
Summary of important points
- Most children with meningococcal disease will become ill enough to require hospital admission within 24 hours of the start of their symptoms. This means there is a narrow window for diagnosis and doctors must be aware of the early symptoms of meningococcal infection to maximise their opportunity to make the diagnosis.
- The symptoms children present with vary with increasing age
- Younger children tend to be brought to hospital earlier in their illness.
- We have identified three important clinical features - limb pain, cold extremities and abnormal colour – which are early sepsis symptoms of meningococcal disease in children and adolescents. We recognise that these symptoms may occur in other febrile illnesses and are not specific to meningococcal disease, but doctors are urged to consider a possible diagnosis of meningococcal disease whenever these symptoms are seen.
- The median times of onset of the early sepsis symptoms were within 7-12 hours. The parents of three-quarters (76.1%) of children identified one or more of these early symptoms before hospital admission. Fewer than 10% of children presented with the classic signs of meningism or impaired consciousness without parents having previously recognised a haemorrhagic rash, or other specific sign of sepsis.
- The rash of meningococcal disease is not an early sign and may not always be present before hospital admission
- The “classic triad” of symptoms of rash, meningism and impaired consciousness generally occur later in the pre-hospital illness. Do not be reassured by the absence of these ‘classical’ features if you see a child within 12 hours of the start of their illness.
The order of progression at all ages is fever, sepsis symptoms and then the classic symptoms of haemorrhagic rash, impaired mental state and meningism
