Nursing assessment: Temp 38.4, HR 172, RR 45, BP 112/50.
Small pin prick rash on abdomen
Ward SHO reviewed child Sleepy but rousable, no neck stiffness or photophobia, HR 171.
No rash but he has a few old chickenpox scars.
Chest clear.
Diagnosis: viral URTI. Child sent home.
Child 3 years old with short history of fever, shaking and generally unwell.
ED Triage assessment:
High temperature, he looks flushed, no rash, unwell child.
Ten minutes later– ED SHO:
Febrile child, listless, irritable and drowsy.
Temp 39.7, HR 170, RR 55.
Pyrexial and drowsy: ? cause, refer to paediatric team.
QUESTIONS ON CASE 2
Q 9 of 12: Could rash be meningococcal?
Yes No
CORRECT : Yes, meningococcal rashes are not always full-blown haemorrhagic rashes. Especially at first, a meningococcal rash may consist of just a few pin-prick petechiae or a blanching macular rash.
Further Information
Examining the Patient
The rash
Most patients with meningococcal septicaemia develop a rash 7242526 - it is one of the clearest and most important signs to recognise. A rapidly evolving petechial or purpuric rash is a marker of very severe disease.
Early stages
In the early stages the rash may be blanching and macular or maculopapular2427 (sometimes confused with flea bites), but it nearly always develops into a non-blanching red, purple or brownish petechial rash or purpura.
Macular rash
Maculopapular rash in meningococcal septicaemia
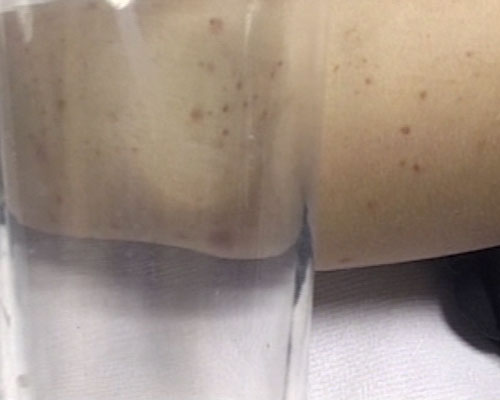
Isolated pin-prick spots may appear where the rash is mainly maculopapular24, so it is important to search the whole body for small petechiae, especially in a febrile child with no focal cause.
Maculopapular rash with scanty petechiae
Rash in ’meningitis’
In meningitis the rash can be scanty, blanching (macular or maculopapular), atypical or even absent.
Very scanty rash: just 3 petechiae on abdomen (2) and chest (1)*
A few petechiae on mottled skin
Spectrum of meningococcal rashes
Meningococcal rashes can be extremely diverse, and look different on different skin types. The rate of progression can also vary greatly.
Petechial rash*
Mixed petechial/ purpuric rash
Mixed petechial/purpuric rash* on freckled skin
Sparse purpuric rash*
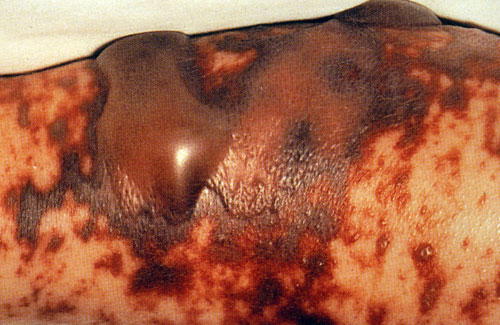
Full-blown purpuric rash of septicaemia
Widespread purpuric rash of septicaemia
Atypical purpuric marks*
Atypical purpuric spots can resemble insect bites
Purple blotches may be larger, resembling bruises*
Purpuric blotches of septicaemic rash can resemble blood blisters
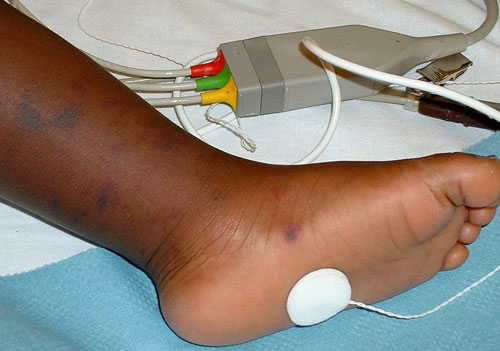
Spotting the rash on dark skin
The rash can be more difficult to see on dark skin, Meningococcal rash on dark skin*
but may be visible in paler areas, especially the soles of the feet, palms of the hands, abdomen, or on the conjunctivae or palate.
Purpuric rash on dark skin - easier to see on sole of foot*
Petechial rash on conjunctivae
Widespread purpuric rash on dark skin^
Advanced Rash
Purpuric areas that look like bruises can be confused with injury or abuse.
Extensive purpuric areas often over the feet, legs and hands are usually called ‘purpura fulminans’.
Purpura fulminans*
Although some of the causes of petechial rashes are self-limiting conditions, many others, including MD are fulminant or life-threatening, and a non-blanching rash should therefore be treated as an emergency519.
It is crucial to remember that the underlying meningitis or septicaemia may be very advanced by the time a rash appears. The rapidly evolving haemorrhagic 'text book' rash may be a very late sign, it may be too late to save the child's life by the time this rash is seen. It is very important to examine children for the signs of meningitis or septicaemia (and raised ICP or shock) and investigate and treat if necessary based on those findings.