|
CASE HISTORY
Hb 11.5, WCC 4.3, Platelets 50.
Na 136, K 3.4, urea 6.2, creatinine 138.
PT (prothrombin time) >180, APTT (activated partial thromboplastin time) >240, INR 12.
Ca 2.1, Mg 0.4

(click for larger graph)
Hb 11.5, WCC 4.3, Platelets 50.
Na 136, K 3.4, urea 6.2, creatinine 138.
PT (prothrombin time) >180, APTT (activated partial thromboplastin time) >240, INR 12. Hb 11.5, WCC 4.3, Platelets 50.
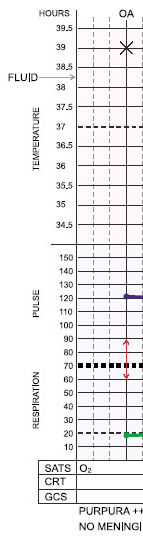
Na 136, K 3.4, urea 6.2, creatinine 138. Diagnosis: meningococcal septicaemia.
Bloods sent for FBC, biochemistry, U&E, clotting.

(click for larger graph)
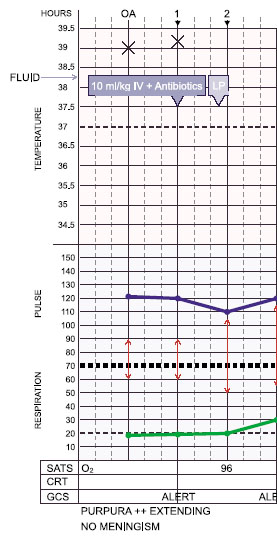
Diagnosis: meningococcal septicaemia.
Bloods sent for FBC, biochemistry, U&E, clotting.

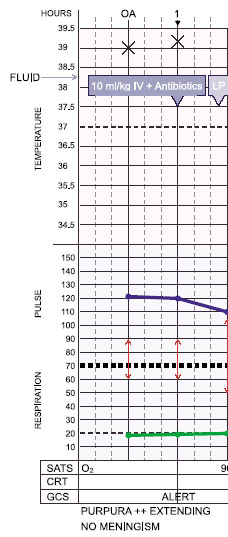
(click for larger graph) Diagnosis: meningococcal septicaemia.
Bloods sent for FBC, glucose, biochemistry, U&E, clotting.
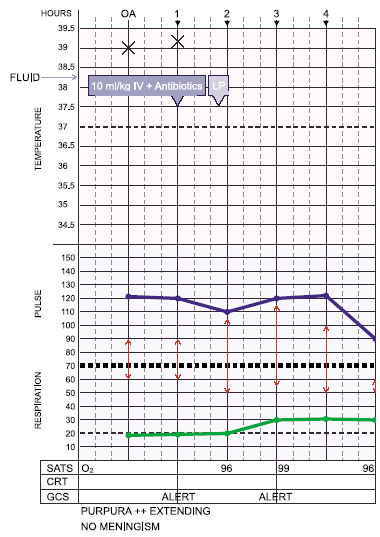
15 year old boy non-specifically unwell for a day. Woke with a widespread purpuric rash and taken straight to hospital.

(click for larger graph)
ED assessment:
Temp 39.0, HR 120, RR 20, BP 90/60.
Alert no meningism; purpuric rash spreading.
|
QUESTIONS ON CASE 4

  Q 9 of 18: is the patient's good conscious level reassuring ?
Q 9 of 18: is the patient's good conscious level reassuring ?
Yes  No No
INCORRECT
: Children and teenagers are able to compensate for loss of blood volume until shock is very advanced, so they can remain alert as blood flow to the brain is maintained at the cost of the other organs.
|
Further Information
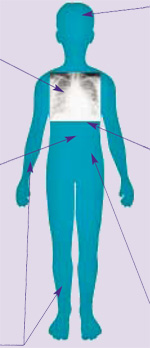
Specific organ dysfunction in shock
Respiratory failure
(arterial PO 2 <10kPa in air or PCO 2 >6)
Common in shock. Capillary leak into lung parenchyma  acute pulmonary oedema. Clinically: tachypnoea, chest wall retraction, hypoxia. |
 |
|
Metabolic derangement
Septicaemia causes profound acidosis and derangements in metabolism, which may affect myocardial function and need correcting. Hypoglycaemia is common. Hypokalaemia, hypocalcaemia, hypomagnesaemia and hypophosphataemia all occur. |
Myocardial failure
Depressed myocardial function is multifactorial, including endotoxin, cytokines, multiple metabolic derangements, hypoxia, and hypovolaemia. Clinically: tachycardia, gallop rhythm, cool peripheries and eventually hypotension.
|
Coagulopathy
(purpuric rash)
Coagulopathy occurs early in patients with septicaemia. The laboratory findings of disseminated intravascular coagulation (DIC) are common in such patients. Coagulopathy is generally associated with the presence of a purpuric rash, but significant coagulopathy may infrequently occur in the absence of purpura. |
Renal failure
Little or no urine output (<1ml/kg/hour) is a very early sign in septic shock, initially due to hypovolaemia. If shock persists then renal failure may occur. Serum creatinine  2 times upper limit of normal for age or 2-fold increase in baseline creatinine indicates renal dysfunction. |
|
|
LOOK IT UP
|