|
CASE HISTORY
Action taken :
- Immediately given antibiotics and 40 ml/kg albumin.
- “Crash call” put out for PICU team.
- Full set bloods taken.
Results:
WCC 2.4, Hb 10.5, pl 70.
Glucose 3.8
Na 149, K 3.4, Ca 2.1, Mg 0.4, PO4 1.6, urea 10.9, Creat 121.
HCO3 15, BE -7.
PT 30, APPT 75, INR 2.5.
Taken to PICU. Still shocked after 40ml/kg. Electively intubated and ventilated, Adrenaline started. Commenced correction of acidosis, K, and Mg.
Extensive purpuric rash developed.
PICU consultant called in to supervise care. 10 month old boy. Taken to GP with h/o sudden onset of fever, vomiting and lethargy for 4 hours. Mother very anxious about child. GP referred child to walk-in clinic at hospital.
History on admission: Feverish and drowsy – sudden onset. 2 episodes of vomiting, 1 soft stool, no rash.
Assessment on admission: Drowsy and pale, dark rings around eyes.
Temp 37.7
CVS: P 181, BP 120/52, CRT 4 secs. Child peripherally shutdown.
RS: RR 32 breathing laboured and child cyanosed.
SaO2 100% in oxygen.
NS: GCS10 then 9, no neck stiffness.
Fine blanching rash on abdo/chest. 1 petechial spot on abdo.
Diagnosis: meningococcal septicaemia
|
QUESTIONS ON CASE 5

  Q 11 of 11: Were there signs of organ failure?
Q 11 of 11: Were there signs of organ failure?
YesNo 
INCORRECT
: Yes -- circulatory/myocardial, respiratory, neurological and renal dysfunction, and coagulopathy.
|
Further Information
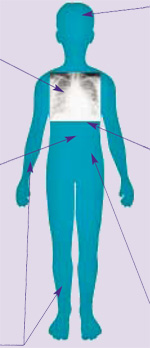
Specific organ dysfunction in shock
Respiratory failure
(arterial PO 2 <10kPa in air or PCO 2 >6)
Common in shock. Capillary leak into lung parenchyma  acute pulmonary oedema. Clinically: tachypnoea, chest wall retraction, hypoxia. |
 |
|
Metabolic derangement
Septicaemia causes profound acidosis and derangements in metabolism, which may affect myocardial function and need correcting. Hypoglycaemia is common. Hypokalaemia, hypocalcaemia, hypomagnesaemia and hypophosphataemia all occur. |
Myocardial failure
Depressed myocardial function is multifactorial, including endotoxin, cytokines, multiple metabolic derangements, hypoxia, and hypovolaemia. Clinically: tachycardia, gallop rhythm, cool peripheries and eventually hypotension.
|
Coagulopathy
(purpuric rash)
Coagulopathy occurs early in patients with septicaemia. The laboratory findings of disseminated intravascular coagulation (DIC) are common in such patients. Coagulopathy is generally associated with the presence of a purpuric rash, but significant coagulopathy may infrequently occur in the absence of purpura. |
Renal failure
Little or no urine output (<1ml/kg/hour) is a very early sign in septic shock, initially due to hypovolaemia. If shock persists then renal failure may occur. Serum creatinine  2 times upper limit of normal for age or 2-fold increase in baseline creatinine indicates renal dysfunction. |
|
|
LOOK IT UP
|